Finance & investing
Investors who search online for information about economic downturns may escalate minor market fluctuations into catastrophic expectations, leading to panic selling. The same algorithmic amplification that surfaces worst-case medical diagnoses also surfaces worst-case financial scenarios, causing disproportionate anxiety about portfolio risk.
Medicine & diagnosis
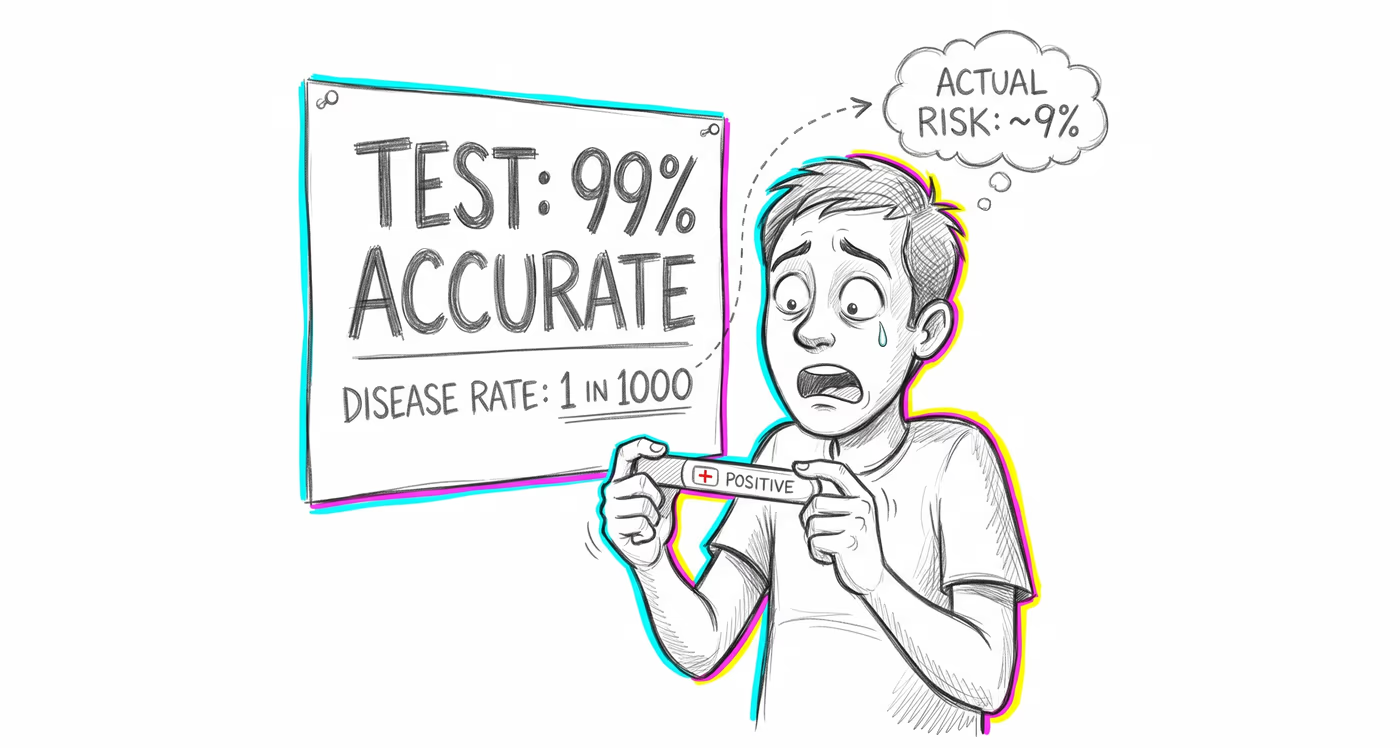
Patients arrive at appointments having already self-diagnosed with rare, serious conditions based on internet searches, leading to demand for unnecessary tests, imaging, and specialist referrals. Clinicians spend significant time de-escalating patient anxiety rather than conducting productive consultations, increasing healthcare costs and reducing system efficiency.